Fluoroscopic-Guided Spinal Injections
• Injects medicine into a part of the spine or in an area near a nerve root.
• Treats problems with the spine but also assists the doctor with the diagnosis.
• Types of injections include:
• Fluoroscopic-guided epidural injections - used for acute and subacute painful spine conditions that create inflammation around spinal nerves.
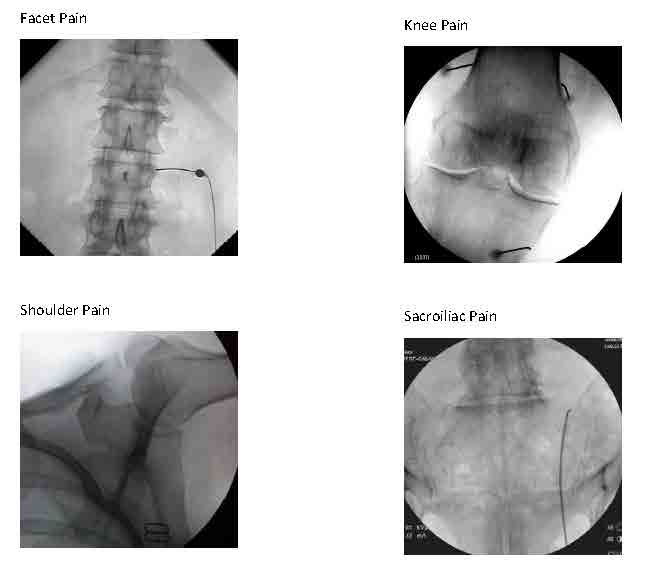
• Fluoroscopic-guided spine joint injections - helpful for spine joint arthritis or spine joint trauma.

Spinal Procedures using Fluoroscopic (X-ray) Guidance
Spinal injections have become essential methods for diagnosing and/or treating spinal pain. The purpose of these injections is to deliver medication, usually a combination of a local anesthetic and a steroid anti-inflammatory medication, to a targeted tissue (like joint, nerve or disc), suspected or known to be a source of pain. The patient’s response to the placement of medication should indicate whether this targeted tissue is a significant source of pain and, if it is, should afford some degree of pain relief. These injections tend to be much more effective in controlling pain and keeping the pain under control than oral medications while avoiding systemic side effects such as gastritis and kidney problems. Pain relief is desirable in and of itself, of course, but it may be just as critical for patients to participate actively in a rehabilitative exercise program supervised initially by physical therapy. For many patients, training spine stabilization through exercise, will be key for safeguarding against having significant recurrent pain, which may ultimately be more of a problem than a transient episode of acute pain.
Before 1990, clinicians performed most injections “blindly,” that is, using anatomic landmarks that can be seen with the eye (observed) and felt with the hands (palpated). Such blind injections can be effective, but may miss the mark in some cases. Since 1990, our practice has been at the forefront of using image guidance to ensure the utmost precision with placement of medication with injections. Now this technologic method is standard practice.
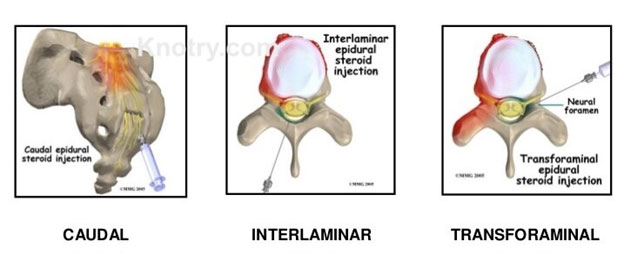
The most commonly employed fluoroscopically guided injections are epidural steroid injections. With x-ray guidance, we can place a potent steroid anti-inflammatory medication in the epidural space that is connected with the spinal canal and the intervertebral discs. This procedure can control inflammation and pain related to the two most common painful conditions that we treat, namely lumbar disc herniations and lumbar spinal stenosis. We can treat cervical (in the neck region) and thoracic (in the mid-back) spinal conditions similarly, but “epidurals” are not commonly needed outside the lumbar spine. The weight of research and our experience bears out a good success rate with disc herniations close to 70%, particularly when there is leg pain (sciatica or radiculopathy) along with back pain. After more than 31 years of experience, we also know that the risks are minimal. Given this success rate and a documented negligible chance of a complication, epidural steroids offer an effective pain control option with minimal risk for disc herniations and most cases of spinal stenosis. The most common technique used is a transforaminal approach to the epidural space in which the injection is placed next to nerve as it exits the spinal canal through a “side door” (foramen). This approach tends to be the most efficient way to deliver the medication and may require placement at two levels or on both sides (bilateral). Alternately, we may opt to use a traditional caudal approach with access through the tailbone. The last approach that is rarely used by us nowadays is the interlaminar approach, which places the injection directly into the central canal between two vertebrae.
Sacroiliac joint (SIJ) pain is a common source of lumbosacral back pain that we can diagnose and treat with 2 types of fluoroscopically guided procedures:
- Sacroiliac joint steroid injections or
- Blocks of nerves to the SIJ with local anesthetic (for diagnosis) twice to determine if blocking long term with Radiofrequency Ablation/RFA (for treatment) is recommended.
Treatment with RFA tends to last around 9 months on average (give or take 3 months), which could be 2-4 times longer than the SIJ steroid injection. However, the steroid injection requires just one session that combines diagnosis and treatment, where the RFA procedure typically requires 3-4 sessions initially. If successful, future treatments with RFA can be repeated generally without the preliminary diagnostic blocks for recurrence of the same pain.

Depiction of a left sacroiliac joint injection
We can diagnose and treat lumbar facet joint pain due to spondylosis similarly, either with a steroid injection into the joint (intra-articularly) or by blocking small nerves to these joints (medial branch blocks) with local anesthetic diagnostically and, if warranted, with RFA therapeutically (as a treatment).
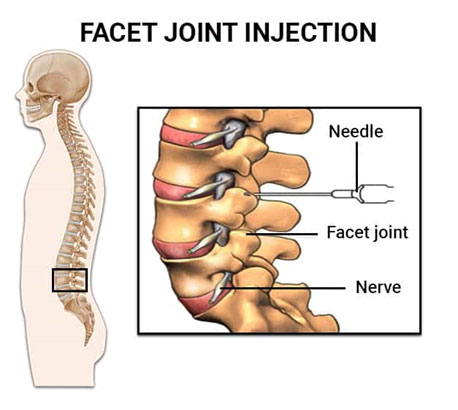
We can use these same approaches to treat facet pain in the neck less frequently and in the midback rarely.
Other procedures using fluoroscopic guidance are evolving. Genicular nerve blocks that involve the usual 2 sets of diagnostic anesthetic blocks followed by blocks with RFA can be very helpful in patients with knee osteoarthritis that is either inoperable or has already failed knee joint replacement surgery. RFA nerve blocks to other joints such as the shoulder and hip for osteoarthritis are in development.
Injections and procedures guided by imaging such as x-ray/fluoroscopy or ultrasound have proven to be more effective with less risk than blind injections. Please refer to the article on ultrasound and ultrasound guided procedures for further information on these other services at Buffalo Spine and Sports Medicine.
Ultrasound-Guided Joint Injections
• Provide direct visualization of various soft tissues.
• Avoid exposing the patient to the risks of radiation.
• Deliver noninvasive, nonionising imaging techniques - allows continuous monitoring of the needle position, facilitating safe and precise cortisone injections.
• Provides soft-tissue imaging capabilities that allow a diagnostic study to be performed before cortisone injection.
Botox Injections for Pain
A breakthrough treatment for many multiple musculoskeletal and neurological conditions. Including:
• Chronic migraine and daily headaches
• Chronic neck and low back pain
• Piriformis Syndrome
• Cerebral palsy with spastic hemi or monoplegia
• Pelvic floor pain and dysfunction
• Temporomandibular and orofacial disorders/ dystonias
• Spastic, painful limb conditions related to stroke, MS, spinal cord injury, Parkinson’s, traumatic brain injury and cerebral palsy
Botulinum neurotoxin (Botox) therapy - For a thorough description, click HERE.
“Because of the multiple levels of my back problems, my doctor wanted me to try an epidural injection. The injection and then the physical therapy made such a difference. I feel so successful that I can get in and out of the car and walk normally. I just keep thinking that this sure beats surgery.” ~ Kristi, patient
Radiofrequency Therapy
• Radiofrequency therapy (RF), also known as Radiofrequency ablation, provides relief for chronic spinal pain, neck, shoulder, hip and knee pain as well as certain types of headaches.
• Pain relief and effectiveness may sometimes take time for the patient to notice the difference, however, it can last between 6 – 12 months and in some cases, years.
• This is a non-surgical, minimally invasive alternative to surgery
• Radiofrequency energy is used to modulate tissue in the peripheral nervous system to help manage chronic pain